Public Policy
Congratulations to CMSNE Public Policy Committee awarded CMSA’s Chapter Excellence and Innovation Award for Public Policy and Advocacy

CMSNE is proud to share that our chapter has been recognized with the Chapter Excellence and Innovation Award for Public Policy and Advocacy at the 2023 CMSA Annual Conference. Special thanks and appreciation to our hard working Public Policy Committee members and advocates.
2023 CM Week Proclamations
Each year, to celebrate Case Management Week, the CMSNE Public Policy committee reaches out to the governors of each state in our chapter to request a proclamation.

New Hampshire

Maine
Vermont

Massachusetts

Congratulations to CMSNE Public Policy Committee awarded CMSNE’s Award of Service Excellence for Public Policy Advocacy

, RN, MSN, MHA, MA, CCM, ACM-RN, CPHM, , RN, BSN, CRRN, CCM, JD, RN, MSN, , MSN, BA, RN-BC and Margaret Flynn, RN, BSN, CCM
Congratulations to CMSNE Public Policy Committee
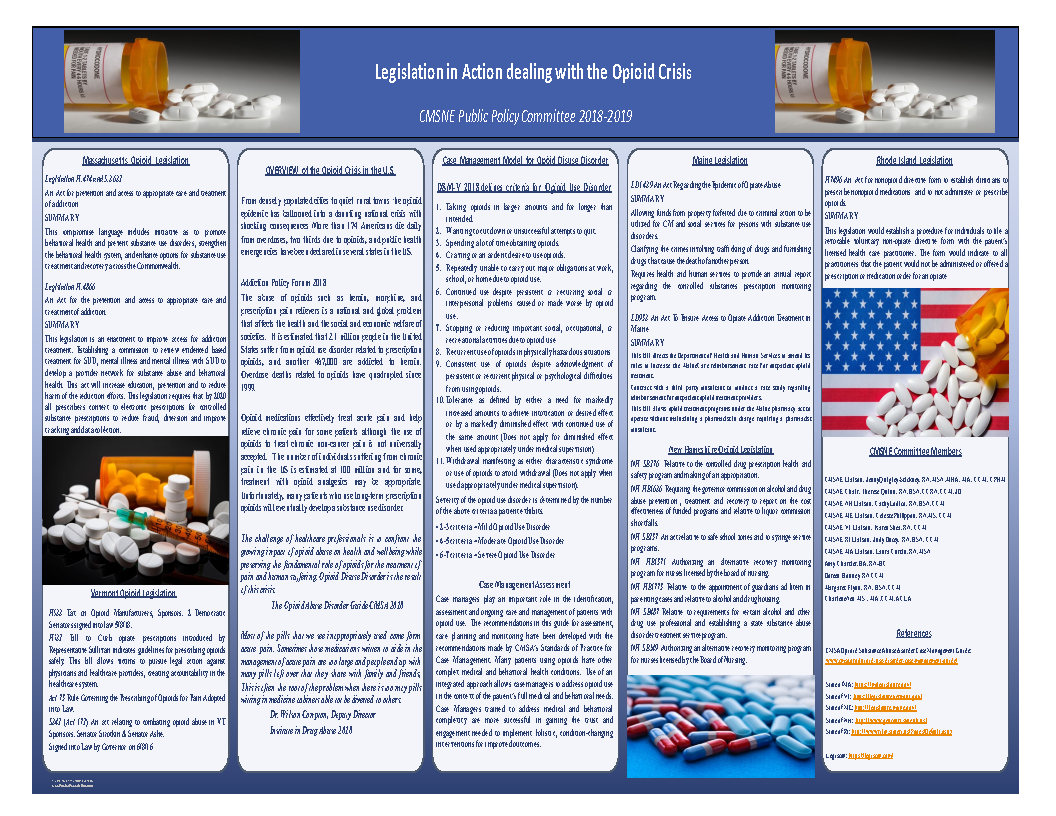
, RN, MSN, MHA, MA, CCM, ACM-RN, CPHM, , RN, BSN, CRRN, CCM, JD, RN, MSN, AND , MSN, BA, RN-BC, all members for the CMSNE Public Policy Committee, were recently published in the CMSA Today, Issue 1 edition, for the article, Legislation in Action Dealing with the Opioid Crisis. To view the article click here.
CMSNE Public Policy update
CMSNE Public Policy Committee has evolved throughout the pandemic to meet the need of an ever change Legislative landscape in an effort to keep both Case management committee members and State legislative members safe. We monitor all legislation via state websites, television, webinar and through Zoom meeting. Our focus has remained the same we are committed to establishing Nurse Licensure Compact in all the New England states. This year 2021Vermont has joined the Compact along with our sister states of New Hampshire and Maine.
Mass and Rhodes Island are still hearing testimony and our committee is hopeful they will join this year. Connecticut has now become a focus in our committee for NLC and we invite all members from this community to work towards the compact.
Nationally the CMSA Public Policy focus has changed targeting legislative efforts Both at the National and State level and incorporating NLC into the support for telehealth legislation.
Telehealth-CMSA supports both state and federal legislation around telehealth and will work collaboratively with other disciplines to understand individual federal and state regulations and updated regulatory actions for healthcare systems and healthcare providers. DOWNLOAD
Mental Health-CMSA is committed to being actively involved in ensuring mental health services are a critical component within the integrated case management model of care. DOWNLOAD
Workforce Development-CMSA is highly committed to workforce development initiatives. The initiatives focus on the case manager, along with the healthcare policies that support the case management role. DOWNLOAD
Congratulations to CMSNE Public Policy Committee
 Winners of 2021 CMSA Chapter Excellence Award for Public Policy and Advocacy. This award pays tribute to the CMSA Chapter offering the most outstanding public policy or advocacy activity. The application submission was based on:
Winners of 2021 CMSA Chapter Excellence Award for Public Policy and Advocacy. This award pays tribute to the CMSA Chapter offering the most outstanding public policy or advocacy activity. The application submission was based on:
The 2020 CMSE Public Policy Committee welcomed new members from the five states within our chapter, including MA, RI, VT, NH, and ME. We have a group of seasoned members who actively participate in our meetings and projects.
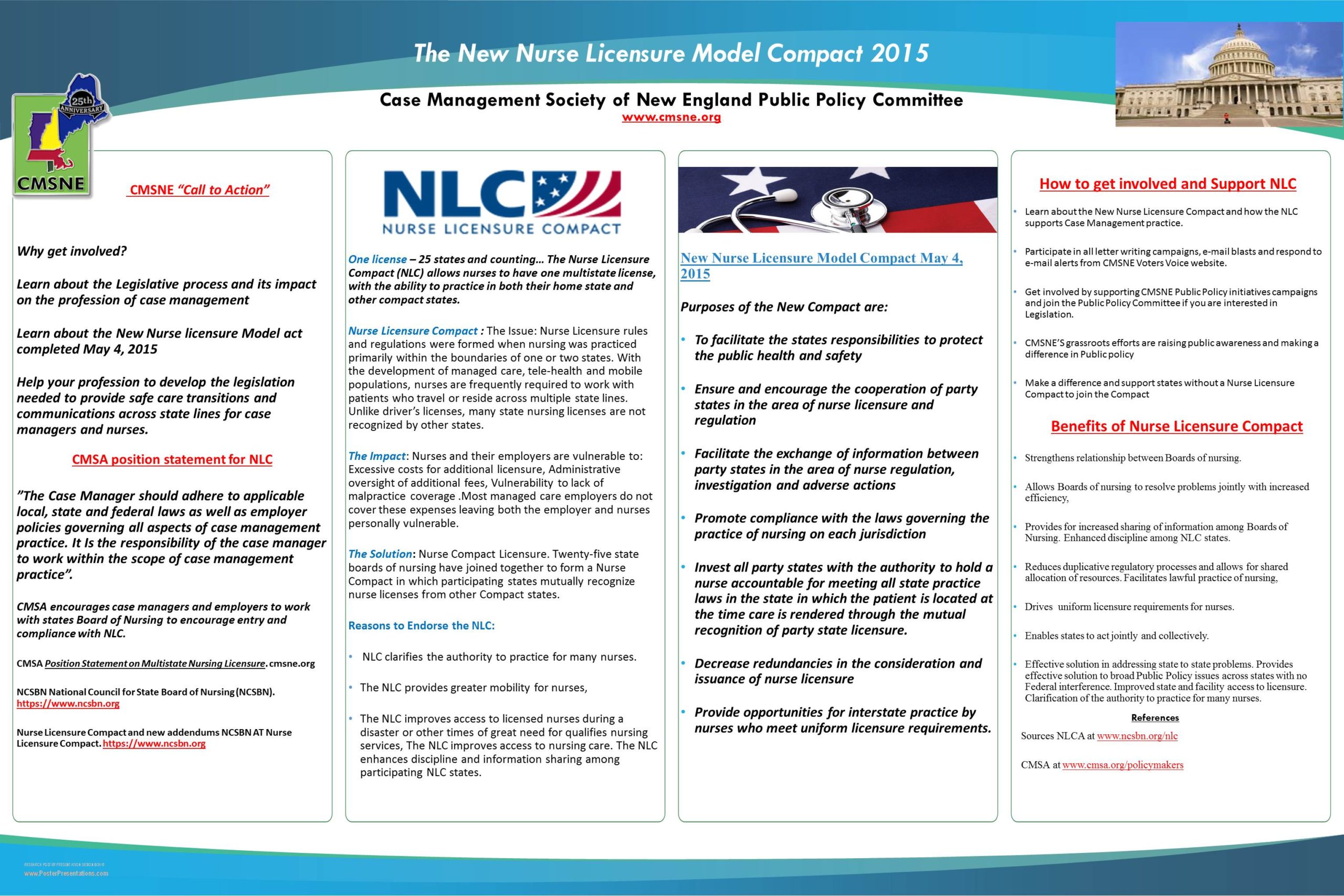
The primary focus of the CMSNE Public Policy Committee has been working to get the Nurse Licensure Compact passed in MA, RI, and VT. To that end, the Public Policy Committee has initiated letter writing campaigns and encouraged phone calls and e-mails to legislators. We have collaborated with lobbyists, the ANA, the MA Hospital Association, AARP, and Fresenius. Since the COVID-19 pandemic caused things to shut down, we were forced to shift gears. Our plan and usual approach is to participate in any legislative hearings pertaining to the NLC, but the pandemic prevented that from happening.
Other initiatives we have been tracking include Telehealth and the Caregiver Act. We can all appreciate how crucial telehealth has become during this pandemic. As a committee, we track legislation in each of the states in New England. Part of the mentoring and education that we practice includes helping individuals become more comfortable with the legislative process by tracking bills as they move to various committees.
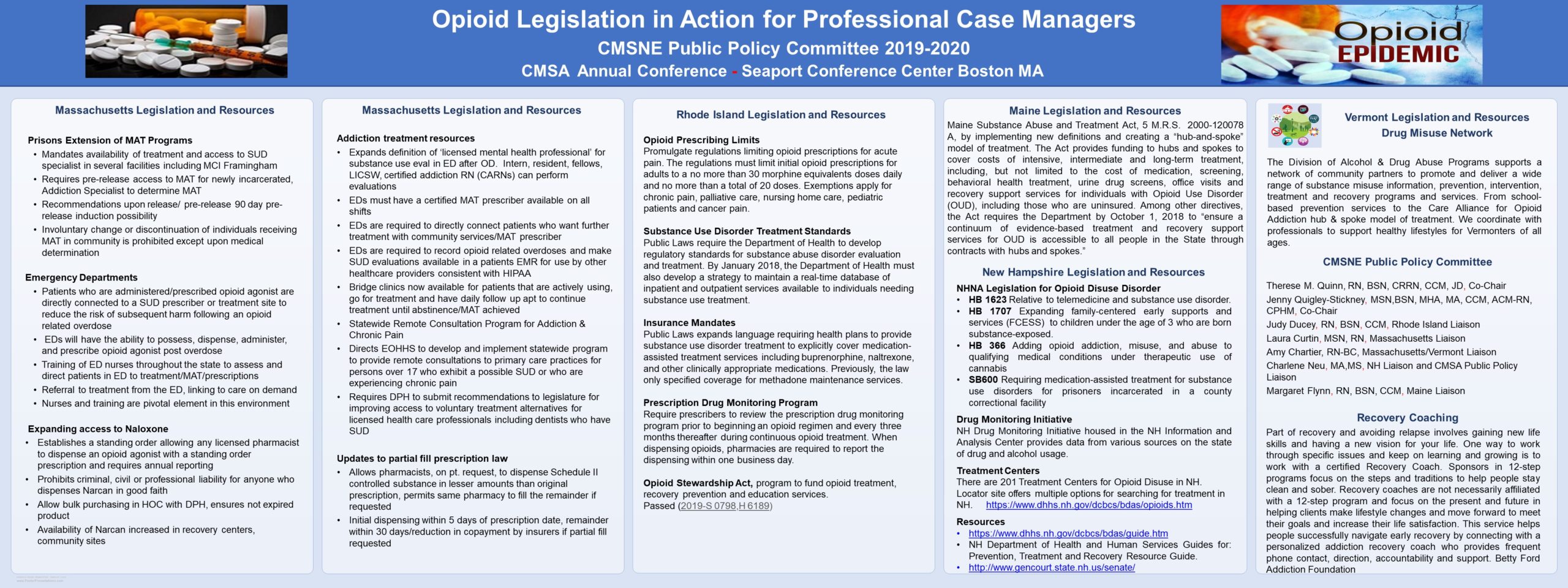
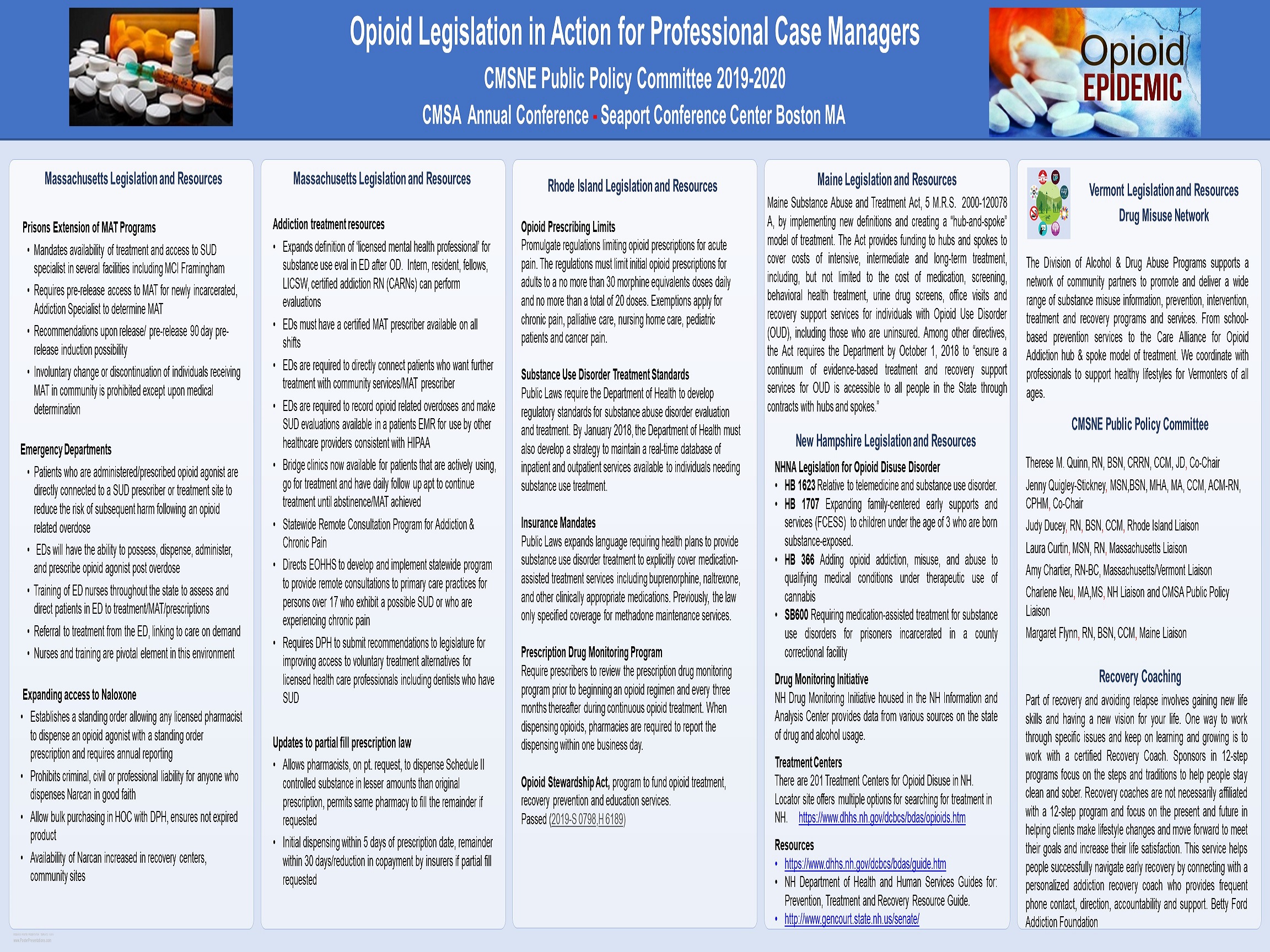
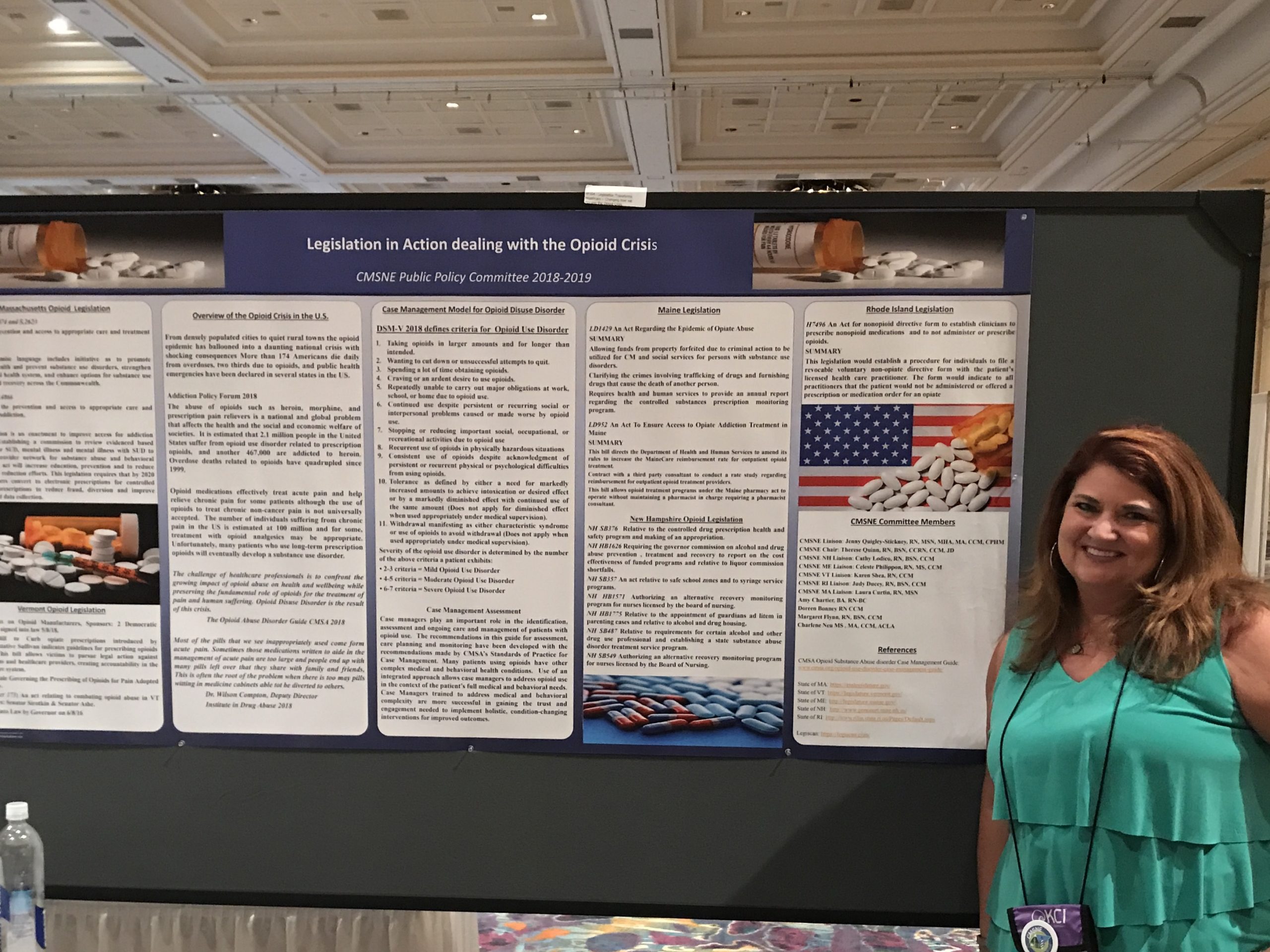
For the CMSA Annual Conference, the Public Policy Committee developed and presented a poster entitled, “Opioid Legislation in Action for the Professional Case Manager. ” This poster served as a follow-up to our previous poster, “Legislation in Action: Dealing with the Opioid Crisis,” which was presented at the CMSA Annual Conference in 2019. While the 2019 poster outlined legislation pertaining to the opioid crisis, the 2020 poster described the programs and actions that resulted from that legislation in each of the New England States. We were asked to submit an article about these posters, initially to be published in the August issue of CMSA Today, but eventually published in the January 2021 issue.
To celebrate Case Management Week, members of the Public Policy Committee reached out to each Governor of the New England States to request a proclamation, and they have been displayed on our website.
Members of the CMSNE Public Policy Committee act as liaisons to the CMSA Public Policy Committee. Updates are provided to the committee to ensure that all members are aware of what is happening with public policy on a national level. We also submit articles to the CMSNE newsletter to provide public policy updates to all members.
During the early months of the COVID-19 pandemic, the Public Policy Committee developed a webinar entitled, “Impact of the Role of the Professional Case Manager Across the Transitions of Care.” This was a 3-part presentation that addressed the role of the professional case manager in different settings during the pandemic, including the acute hospital setting, the community/workers’ compensation, and in gerontology. We also addressed the virus itself, statistics, as well as safety precautions, PPE, testing, and treatment. We provided resources for self care and resilience and some ethical considerations. This program offered CEUs and was well-received.
For committee article publication. , RN, MSN, MHA, MA, CCM, ACM-RN, CPHM, , RN, BSN, CRRN, CCM, JD, RN, MSN, AND , MSN, BA, RN-BC, all members for the CMSNE Public Policy Committee, were recently published in the CMSA Today, Issue 1 edition, for the article, Legislation in Action Dealing with the Opioid Crisis. To view the article click here.
Cmsne public policy poster presented at 2023 cmsa conference
|
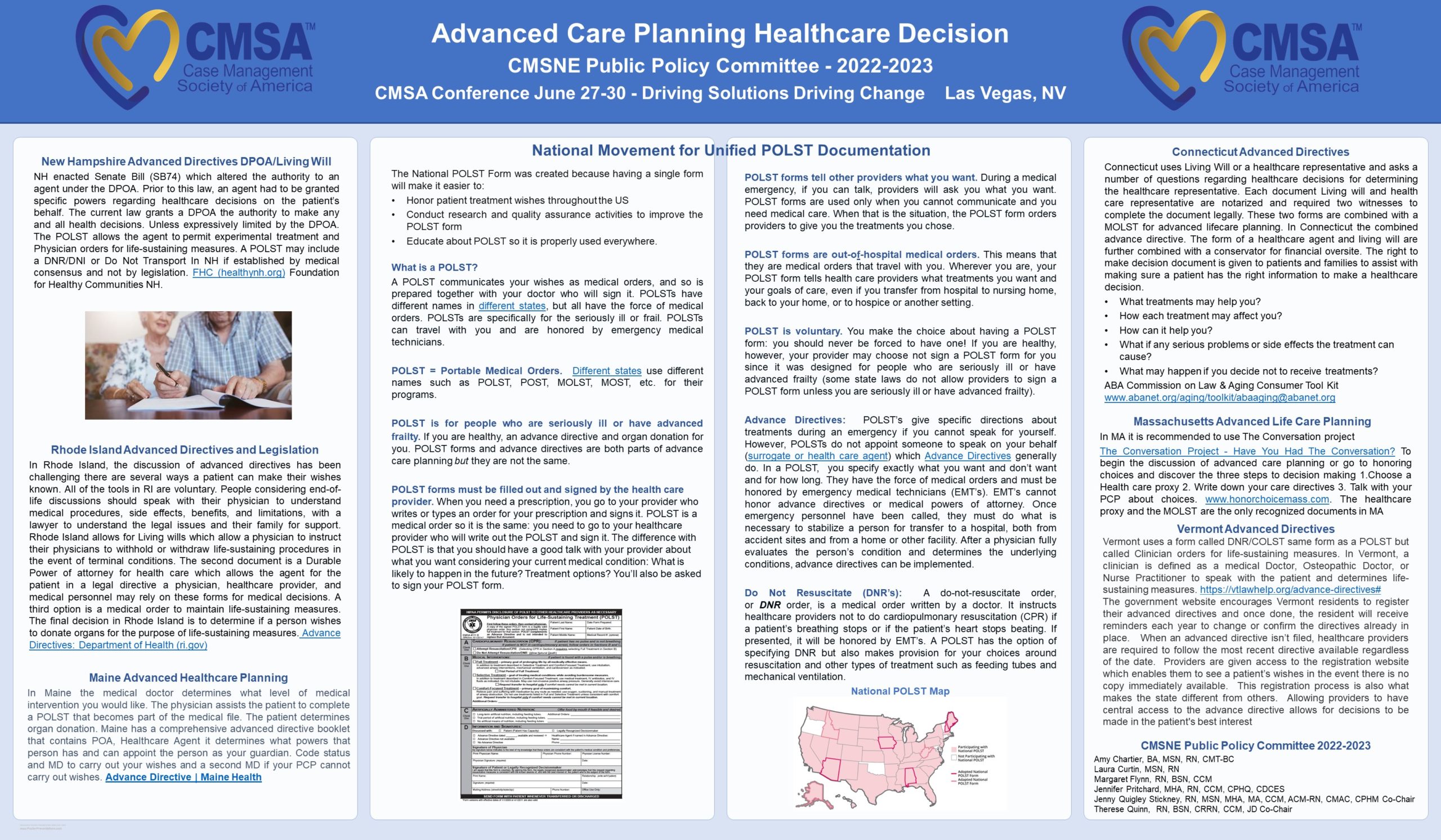
Advanced Care Planning Healthcare Decision |
Cmsne public policy posters presented at 2021 cmsa conference
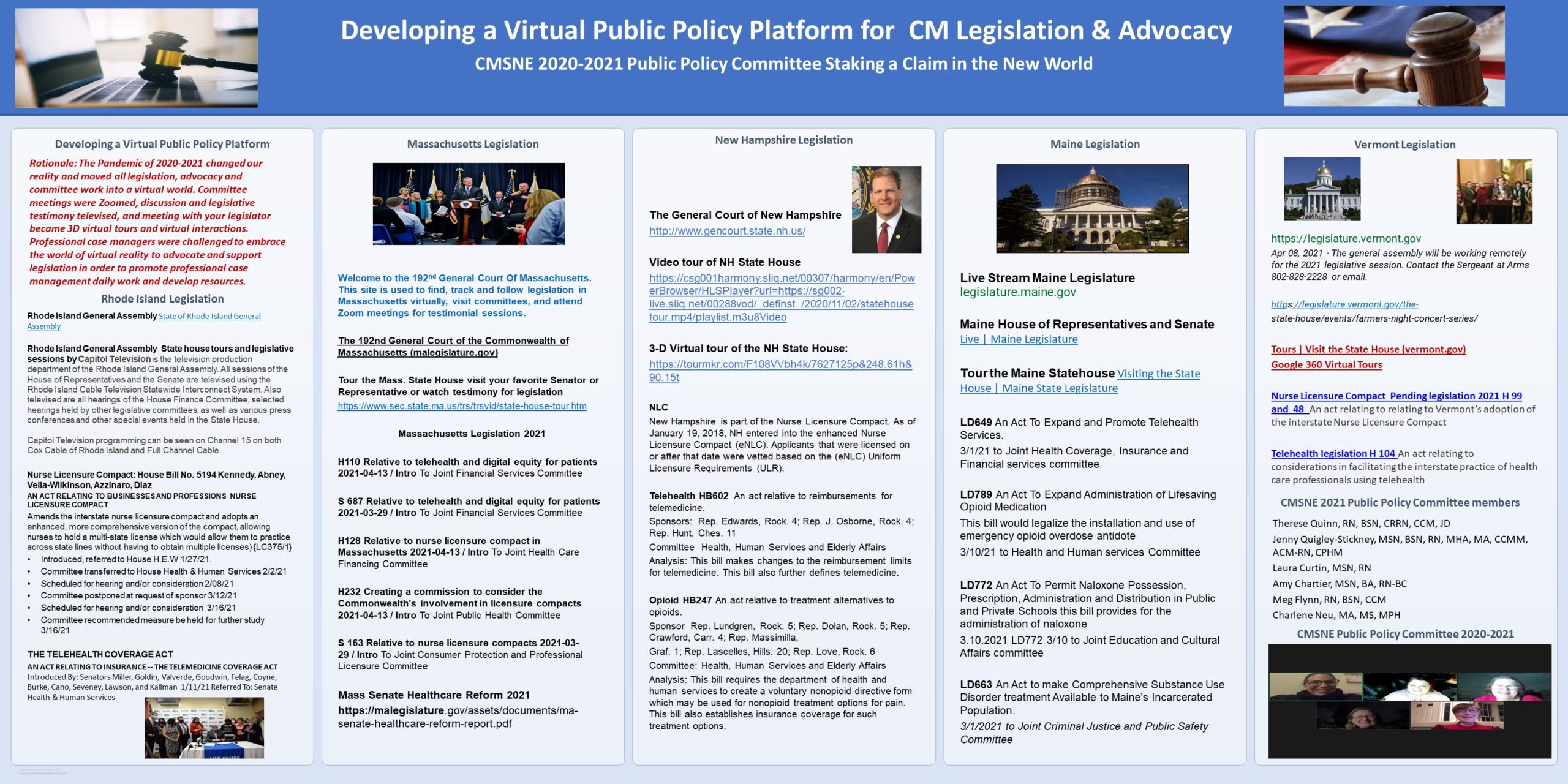
The Pandemic caused many to embrace the virtual world in order to go about their usual business, including accessing health care. Advocacy became crucial to ensure all were able to access needed care. The Public Policy Committee of the CMSNE created two posters to assist care managers to navigate the legislative process nationally, and in their respective states, to enabled them to keep current regarding legislation that affected their practice of case management.
|
Developing a Virtual Public Policy Platform for CM Legislation & Advocacy .
|
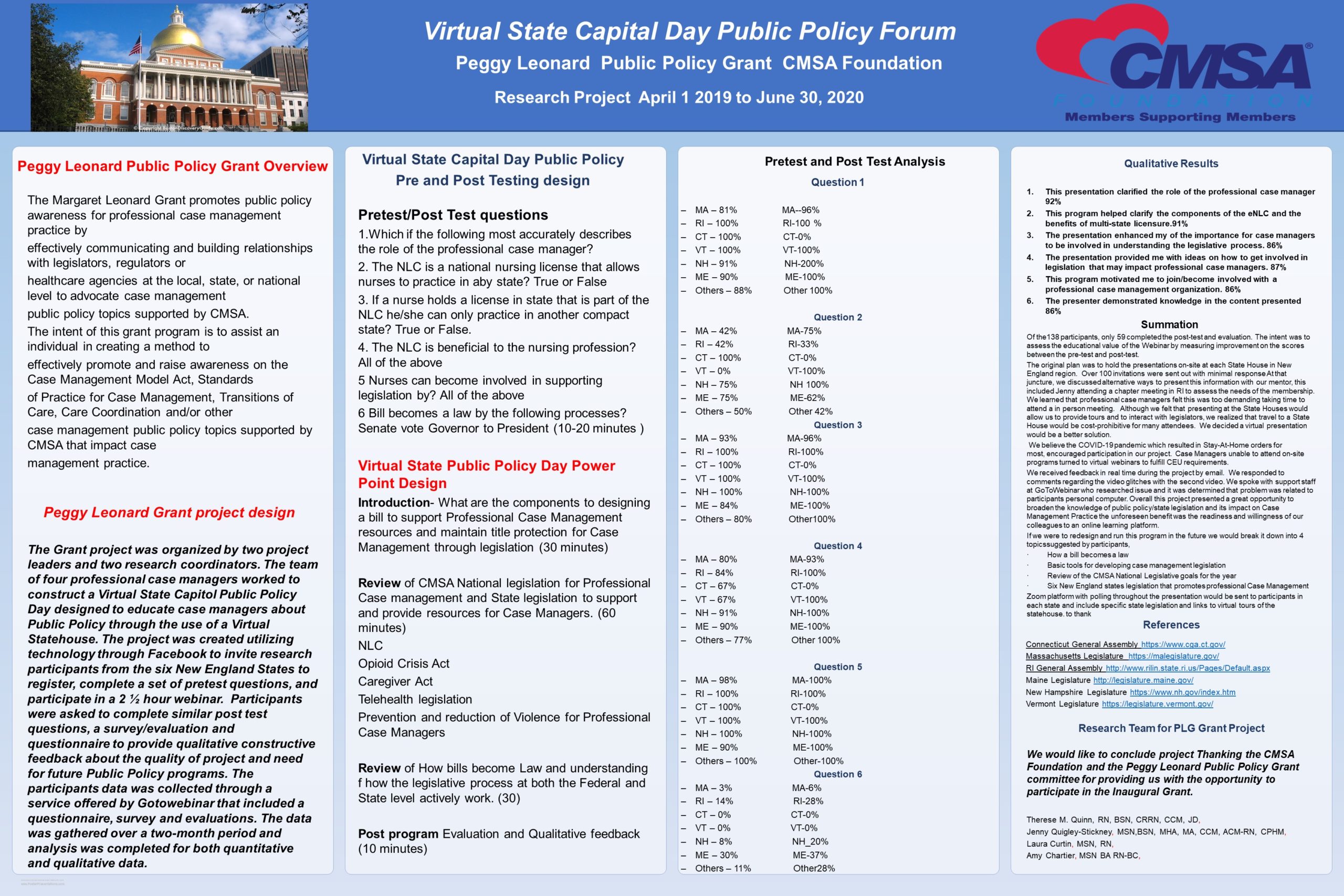
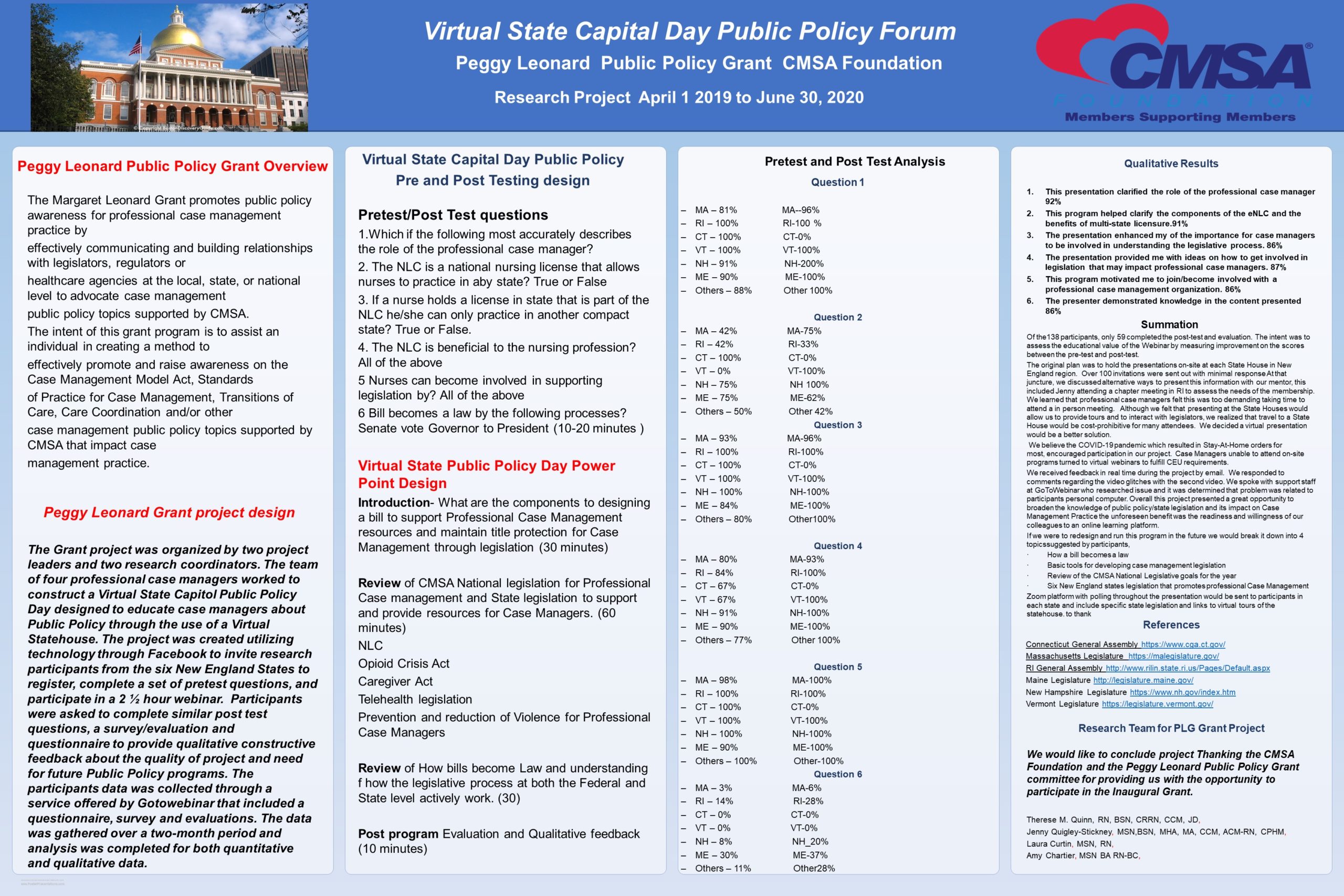
Virtual State Capital Day Public Policy Forum – Peggy Leonard Public Policy Grant CMSA Foundation
|

Public Policy Posters Throughout the Years
Tour Public Policy posters created by CMSNE members from over the years that were displayed at local and national conferences.







Click on images to enlarge for enhanced viewing.
Understand how NLC impacts Nursing
Click below to watch NCSBN’s “Unlocking Access to Nursing Care across the Nation,” a half-day forum that brought expert panelists from across the U.S. together to discuss the challenges of 21st century nursing and the solutions presented by the enhanced Nurse Licensure Compact (NLC). (update from NCSBN)
NLC Articles supporting the rationale for forming a Nurse Licensure Compacts:
Five Reasons to Endorse the NLC
The Enhanced Nurse Licensure Compact – What Policymakers Need to Know
For additional information or interest in participating on CMSNE’s Public Policy Committee contact the chapter office at cmsne@comcast.net
Virtual State House Tours
Due to Covid 19 protocols, most New England state houses have offered virtual tours in addition to on-site tours. These links are easily found if state house webpages, usually with the visit or tour information. With the availability of online tours, many can visit their state houses without having to worry about parking, commuting, and/or close contact. This option also allows access to tour to those who otherwise may not be able to visit in person.





